By: Laney Herndon & Carmen Maria Canino
The group began their day at 9 am at the Bunk Hotel Cafe. The most popular breakfast today was a dish called “Smash!” which was two poached eggs with smashed avocado on a piece of toast.
After breakfast, the group caught a train to Deventer, a place where Paul once studied and worked. We walked around town and Paul showed us his old fraternity house where he was once the president. The town contained many historical buildings that were beautifully decorated. The center of the town has a gigantic fountain with detailed angel statues, and there were many small shops and restaurants surrounding that area.



We ended our tour of the town at the University of Saxion of Applied Science. We were welcomed to a beautiful meeting room with complimentary coffee, tea, and biscuit snacks. About 20 Dutch nursing students met us in the meeting room shortly after we arrived. Professor Ingrid gave us a brief presentation on the Optimizing Palliative Care Education project. She explained that this project aims to educate upcoming nurses and doctors about palliative care and pain management methods. Currently, the Netherlands has a program to educate students who are studying palliative care, and this program also offers continuing education on this topic for medical practitioners that are already licensed. The course is based on a book called Quality Framework Palliative Care Netherlands (2017). Some of the themes in the palliative care management are sharing decision management, advance care planning, symptom managements, euthanasia, palliative sedation, and interprofessional collaboration.


The Dutch and Dickinson students were divided into four groups for a “speed dating” activity. In each of these groups, specific euthanasia/the end-of-life topics were discussed. Some of the topic discussed were: private/public insurance and how that influences the end-of-life care quality, euthanasia versus palliative sedation, Dutch students’ experience as a home care aid, the Dutch perspective on aging and dying, the work quality as nurses in Netherland, and more. In our discussions with the students, I found that many of them prefer palliative sedation over euthanasia because of the easier access to this type of care. Sometimes, the euthanasia process can last months and even years while palliative sedation is offered during the last two weeks of a patient’s life. Interestingly, euthanasia is covered under the basic insurance package in the Netherland, so people from all socioeconomic background have equal access to it. However, only Netherland citizens have access to euthanasia. Furthermore, Dutch students also feel much more trusting towards their general practitioner due to the doctor’s often close relationship with the patient and their family. They feel like they would be comfortable to talk about the end-of-life topics with their doctors.



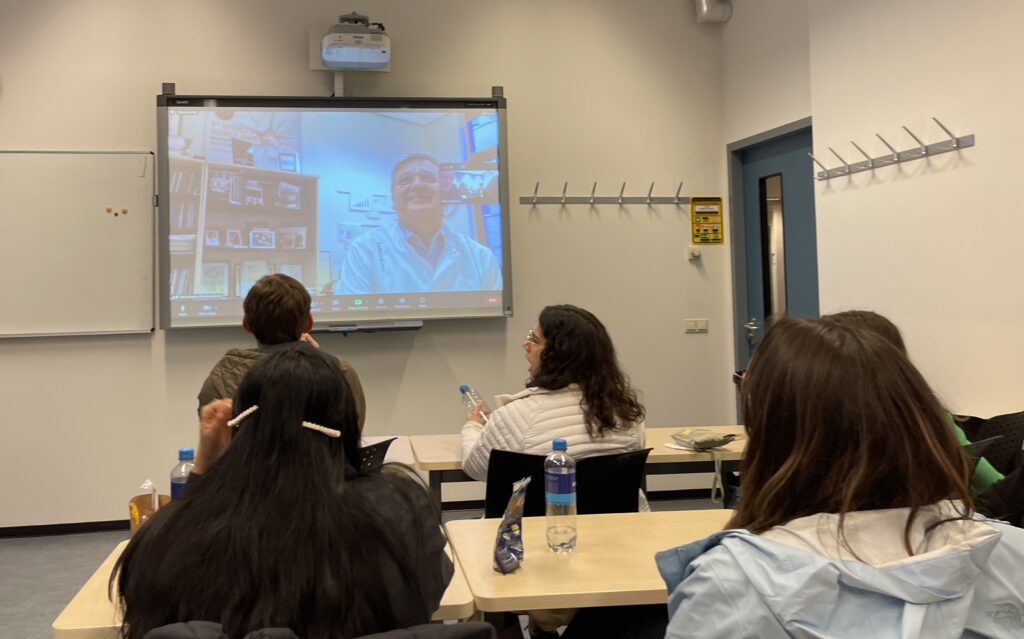
After talking to the Dutch students, we moved to another classroom to meet with Dr. Kris Vissers. He is a pain and palliative care specialist who has experience in emergency medicine, intensive care medicine and anesthesiology. We were on a zoom meeting with him for two hours, and he was able to answer and explain many palliative care, palliative sedation, and euthanasia questions our class had. Palliative care is relatively new in Netherland, and it was introduced around 1994. This type of care is now widely accepted in Netherland. Dr. Vissers further explained that only about 4% of patients receive euthanasia every year. In our class, there was a lot of confusion surrounding the topic of palliative sedation and how it differs from getting morphine drip treatments. Dr. Vissers explained that morphine is not part of palliative sedation. Palliative sedation is often treated with Midazolam, a drug that can induce unconsciousness state in patients to alleviate “annoying” symptoms. Palliative sedation can alter a patient’s conscious state by titrating the drug concentration given to the patient. This can be especially helpful for some patient. For example, some Muslim patients may want to be woken up at certain times, so palliative sedation can be lifted during those moments. This way, they are awaken to be with their family to pray to Allah each day. Other patients want low dosage of Midazolam so that they can be semi-conscious, but their negative symptoms from their disease is lessened or eliminated. This is often the best-case scenario for the family, so they can interact with the patient during their last few days.
Our day ended with traveling back to Utrecht via the train system. Today was incredibly educational and rewarding because we were able to have personal interactions with Dutch students, professors, and doctors on the topic of death and dying.

Leave a Reply